
It actually makes me itch just thinking about it; mites burrowing into the skin and laying eggs. And then to think the mites are also leaving fecal deposits in these burrows in the skin.

These burrows are tiny threadlike projections, ranging from 2 mm-15 mm long that appear as thin gray, brown, or red lines in affected areas. The burrows can be very difficult to see.
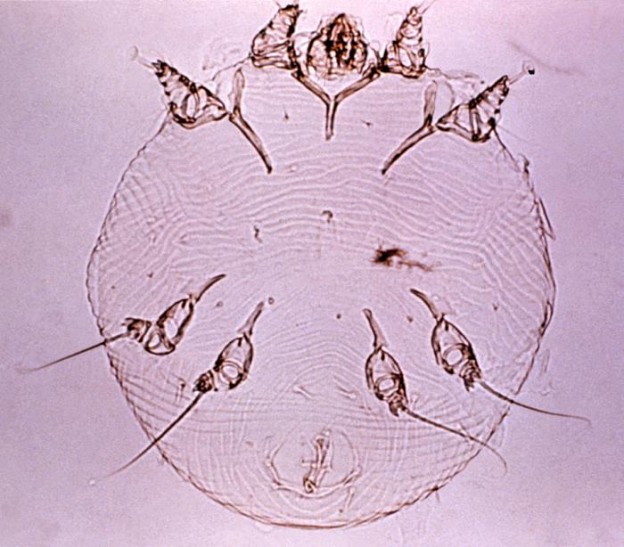
Scabies is caused by an infestation by the eight-legged “itch mite”, Sarcoptes scabiei.
Transfer of this mite from person to person typically occurs through prolonged direct contact with infested skin and also during sexual contact. In fact, sexual contact is the most common form of transmission among sexually active young people.
Transfer from undergarments and bedclothes occur only if these have been contaminated by an infested person immediately beforehand.
Outbreaks have happened in nursing home and similar institutions, albeit rare.
It may take up to two months for symptoms to appear after initial infestation. Scabies produces skin rash composed of small red bumps and blisters and affects specific areas of the body.
Lesions are prominent around finger webs, wrist and elbows, armpits, belt line, thighs and genitalia of males and nipples, abdomen and buttocks are frequently affected in women. In infants; the head, neck palms and soles may be involved.
Itching is intense, especially at night and complications due to secondary bacterial infections with staph and strep are possible.
Then there is the more severe form is called Norwegian scabies, or crusted scabies. According to Dr. Melissa Conrad Stöppler, there seems to be a problem with the immune response to the mites, allowing for the infestation of an individual with hundreds of thousands of the mites. Crusted scabies almost always affects people with a compromised immune system and is observed most frequently in the elderly, those who are mentally or physically disabled, and in patients with AIDS, lymphoma, or other conditions that decrease the effectiveness of the immune response.
The lesions of this distinctive form of scabies are extensive and may spread all over the body.
Human scabies is caused by a different parasite than that that causes mange in animals. When canine or feline mites land on human skin, they fail to thrive and produce only a mild itch that goes away on its own.
Diagnosis is made based upon the appearance and distribution of the rash and the presence of burrows. Whenever possible, scabies should be confirmed by isolating the mites, ova or feces in a skin scraping. Scrapings should be made at the burrows, especially on the hands between the fingers and the folds of the wrist.
Scabies can be treated by using a scabicide like 5% permethrin, 10% Crotamiton or 1% lindane. There are no over the counter medications that are approved to treat scabies.
The Centers for Disease Control and Prevention recommend the following to prevent and control scabies:
Scabies is prevented by avoiding direct skin-to-skin contact with an infested person or with items such as clothing or bedding used by an infested person. Scabies treatment usually is recommended for members of the same household, particularly for those who have had prolonged skin-to-skin contact. All household members and other potentially exposed persons should be treated at the same time as the infested person to prevent possible reexposure and reinfestation.
Bedding and clothing worn or used next to the skin anytime during the 3 days before treatment should be machine washed and dried using the hot water and hot dryer cycles or be dry-cleaned. Items that cannot be dry-cleaned or laundered can be disinfested by storing in a closed plastic bag for several days to a week. Scabies mites generally do not survive more than 2 to 3 days away from human skin. Children and adults usually can return to child care, school, or work the day after treatment.
Persons with crusted (Norwegian) scabies and their close contacts, including household members, should be treated rapidly and aggressively to avoid outbreaks. Institutional outbreaks can be difficult to control and require a rapid, aggressive, and sustained response.
Rooms used by a patient with crusted scabies should be thoroughly cleaned and vacuumed after use. Environmental disinfestation using pesticide sprays or fogs generally is unnecessary and is discouraged.
Article originally published June 2009

I’ve been struggling with this nightmare for so long… I tried everything over the counter but am now going to go all out with the prescription stuff. Thank you for posting about this.